In the realm of internal fixation, the Herbert Screw—a headless, cannulated compression screw—represents a paradigm shift in treating intra-articular fractures. Originally designed by Timothy Herbert for scaphoid fractures, the technology has evolved into a versatile tool for small bone osteosynthesis. Unlike traditional bone screws, the Herbert screw features differential thread pitches at its proximal and distal ends. This mechanical ingenuity allows the screw to provide interfragmentary compression as it is driven into the bone, without the need for a prominent screw head that could irritate soft tissues or interfere with joint articulation.
As the global medical device market shifts towards Minimally Invasive Surgery (MIS), the demand for high-precision Herbert screws has skyrocketed. Today, selecting a "Top 10" supplier is not merely about price; it is about evaluating biocompatibility, thread precision, and supply chain reliability. This guide delves into the technical benchmarks that define the industry leaders and explores why the fusion of clinical experience and advanced manufacturing is critical for surgical success.
The next generation of Herbert screws is moving toward magnesium alloys and PLLA. These materials provide initial stability and slowly degrade, eliminating the need for a second surgery to remove the implant.
Leveraging CT-guided data, factories are beginning to produce patient-specific screw lengths and thread profiles, ensuring perfect anatomical fit for complex comminuted fractures.
Manufacturing is aligning with robotic-assisted surgery. Future screws will feature smart-heads for easier engagement with robotic arm drivers, reducing operative time and radiation exposure.
The concentration of orthopedic manufacturing in China—specifically in hubs like Changzhou and Suzhou—has created an unparalleled ecosystem. Factories like KaiSo (established 2004) leverage this cluster effect to provide significant Information Gain for global buyers. This includes:
China accounts for nearly 40% of the world's orthopedic implant manufacturing. The efficiency is driven by high-speed CNC Swiss-type lathes capable of machining Herbert screws with sub-micron tolerances.
Leading suppliers now offer comprehensive MDR (Medical Device Regulation) documentation, providing localized support for clinical trials and regulatory registration in the EU and Americas.
KaiSo has established a complete Quality Assurance System to continuously fulfill the requirements according to ISO9001, 13485, and CE. Their facility spans 29,523㎡, integrating automated production processes with rigorous human oversight.










Registration: 2004-11-03
Floor Space: 29,523 ㎡
Industry Years: 22 Years
QA/QC Inspectors: 69
R&D Engineers: 59
Certifications: ISO 13485, CE, MDR
South America: 30%
Southeast Asia: 20%
Western Europe: 20%
The versatility of Herbert screws extends across various orthopedic sub-specialties. Understanding these scenarios is key for clinical procurement:
The primary use case. The headless design allows the screw to be buried beneath the cartilage of the wrist, facilitating early range of motion without impingement.
Used in the knee and elbow to fixate small bone fragments within the joint capsule where a traditional screw head would destroy articular surfaces.
Ideal for PIP or DIP joint fusion in the fingers, providing strong compression to ensure high fusion rates in geriatric populations.
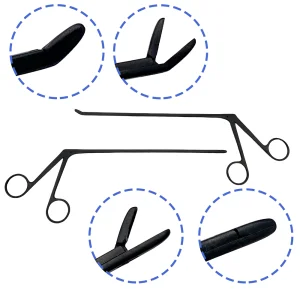
The Herbert screw is headless and cannulated. Its headless design allows for intra-articular (inside the joint) placement without damaging the opposing cartilage. The cannulation allows for precise placement over a guide wire.
The leading (distal) thread has a larger pitch than the trailing (proximal) thread. As the screw turns, the distal part moves into the bone faster than the proximal part, effectively drawing the two bone fragments together.
For international markets, ISO 13485 is mandatory. For the European market, CE marking under the new MDR (Medical Device Regulation) is crucial. FDA 510(k) is required for the US market.
Yes, but with caution regarding growth plates. Surgeons often choose smaller diameters (1.5mm or 2.0mm) for pediatric small bone fixation.
Titanium Grade 5 ELI offers superior biocompatibility, a lower modulus of elasticity (closer to bone), and is MRI-compatible, which is essential for post-operative imaging.